
Files
Download Full Text (377 KB)
Publication Date
4-29-2020
Disciplines
Internal Medicine
Description
Introduction: • Nocardia is known to cause severe pulmonary or disseminated infection in immunocompromised patients, but can cause infection in immunocompetent patients. Providers should consider Nocardiosis in immunocompetent patients with prolonged and unexplained respiratory failure. • The preferred therapy for pulmonary Nocardiosis is a sulfa antibiotic for 3-6 months. Toxicity from prolonged use of alternative agents presents a therapeutic challenge in those with sulfa allergy.
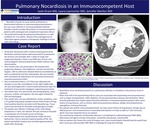
Case Report: • An 85 year-old woman with a history of paroxysmal atrial fibrillation and heart failure with preserved EF presented to her primary care provider with 1 week of cough and progressive dyspnea. Chest x-ray (CXR) was normal, and echocardiogram demonstrated known HFpEFwithout new abnormalities. • Two months later, she presented to the hospital with progressive dyspnea, chest tightness, and was found to be hypoxic. CXR on admission showed bilateral consolidations as well as mediastinal and hilar adenopathy. She was treated with ceftriaxone & azithromycin for presumed community-acquired pneumonia (CAP). • Due to treatment failure, a CT Chest was obtained and showed a mass-like consolidation in the right middle lobe; she was discharged with a several-week prednisone taper for treatment of presumed cryptogenic organizing pneumonia. • Two weeks later, she returned for worsening dyspnea, chest pressure, malaise, and hypoxia. She was again treated for CAP and discharged. • One month later, she was admitted for similar symptoms, and a CT-guided lung biopsy showed several small clusters of long Gram-positive bacteria consistent with Nocardia spp. Tissue culture was positive for Nocardia cyriacigeorgicacomplex. • The patient was offered a challenge of her sulfa allergy (reported as a rash), but refused. She was started on linezolid in anticipation of a 6 month course of therapy. • Her hospitalization was complicated by cardiac & renal dysfunction. Due to severely impaired quality of life, the patient elected for hospice care and died approximately 2 weeks after discharge.
Discussion: • Nocardiosis most commonly presents as a pulmonary infection as inhalation is the primary route of exposure. • More than half of all reported Nocardiosis cases are associated with preexisting immunocompromise such as organ transplantation, AIDS, diabetes, chronic granulomatous disease and alcoholism. More recently published case reports depict Nocardia infections in immunocompetent patients with a prior history of lung disease, such as chronic obstructive pulmonary disease, allergic bronchopulmonary aspergillosis, and bronchiectasis. • Our patient was neither immunocompromised, nor had a prior history of lung disease, though was an elderly person. Immunosenescenceis associated with decline in innate as well as T-cell immunity, which may have imparted risk to our patient. • The mainstay for treatment of Nocardia infections is trimethoprim-sulfamethoxazole (TMP-SMX). Alternative oral agents include minocycline, amoxicillin-clavulanate, and linezolid. • Had our patient not chosen the route of hospice care, close monitoring for linezolid toxicity would have been necessary with possible TMP-SMX re-challenge for long term therapy.
Department
Internal Medicine
Department
Graduate Medical Education
Conference / Event Name
Academic Achievement Day, 2020
Location
Providence St. Vincent, Internal Medicine Residency, Portland, Oregon
Recommended Citation
Grant, Leah; Loertscher, Laura; and Marfori, Jennifer, "Pulmonary Nocardiosisin an ImmunocompetentHost" (2020). Providence St. Vincent Internal Medicine 2020. 7.
https://digitalcommons.providence.org/psv_internal/7



